
Cottages C and D - Massillon State Hospital
Cottage Plan Architecture
The following text is taken from a Wikipedia article on Asylum Architecture (under Creative Commons Attribution-ShareAlike License)
Asylum and hospital architecture in the United States, including the architecture of psychiatric hospitals, affected the changing methods of treating the mentally ill in the nineteenth century: the architecture was considered part of the cure. Doctors believed that ninety percent of insanity cases were curable, but only if treated outside the home, in large-scale buildings. Nineteenth-century psychiatrists considered the architecture of asylums, especially their planning, to be one of the most powerful tools for the treatment of the insane, targeting social as well as biological factors to facilitate the treatment of mental illnesses. The construction and usage of these quasi-public buildings served to legitimize developing ideas in psychiatry. About 300 psychiatric hospitals, known at the time as insane asylums, were constructed in the United States before 1900. Two prominent architectural design strategies, associated with the medical philosophies of the time, were the Kirkbride Plan and the Cottage Plan.
The Kirkbride Plan
The Quaker reformers, including Samuel Tuke, who promoted the moral treatment, as it was called, argued that patients should be unchained, granted respect, encouraged to perform occupational tasks (like farming, carpentry, or laundry), and allowed to stroll the grounds with an attendant and attend occasional dances. While the moral treatment could, with difficulty, be employed in an old house or adapted almshouse, this situation was considered a sad compromise. In the United States, doctors developed a highly specialized building type for 250 patients. Dr. Thomas Story Kirkbride devised a widely applicable set of planning principles that ensured classification by type of illness, ease of surveillance, short wards for good ventilation, and clarity of circulation.
The buildings helped establish psychiatry as a profession, because the asylum was the only setting for the practice of psychiatry in the nineteenth century, there were no out-patient visits, no doctors’ offices. Professional medical journals were replete with articles on architecture, a constant preoccupation for the asylum superintendent, and architects ventured opinions about the proper classification of patients.
The Cottage Plan
The Kirkbride plan, also called the linear plan, dominated asylum building. It tended to produce very large, long structures. By the middle of the nineteenth century, some doctors complained that large monolithic asylums had not lived up to their expectations. But psychiatrists did not immediately abandon their belief in the therapeutic environment; instead, they argued for a different therapeutic environment. Clinging to a belief that architecture influenced human conduct, they proposed smaller cottage-like structures to replace the Kirkbride-plan hospitals. These cottages were to be arranged in a village, an homage to the Belgian town of Gheel, where citizens looked after mentally ill people who for centuries gathered there to worship at the shrine of St. Dymphna, the patron saint of lunatics. Dr. John Galt romanticized this medieval model as an ideal setting for the cure of the disease, thus causing a rift among the self-named “brethren” of asylum superintendents.
The cottages varied in size from those which accommodated six to a dozen patients to larger ones which accommodated 20 or more. They were usually constructed either in groups or along streets and avenues as a village. In the group arrangement, the several groups were given up to a particular industry as a farm group, where the patients were employed at farming, and others, as the garden, the brick yard, shop industries, etc., all of these being a part of one institution on a single large estate. In the village plan, the institution was laid off in streets and avenues, and had the appearance of an ordinary village, each cottage having a flower garden in front, shade trees, etc. In either plan, there was conveniently located near the center of the plant an administration building, a hospital for the sick and those requiring special care, a bakery, a laundry and other utility buildings. The cost of construction was small as compared with older plans of asylum construction.
This approach was viewed as more homelike, more convenient for administration and as permitting indefinite expansion.
by Wayne Carlson ©2016
Grandview Heights/Marble Cliff Historical Society
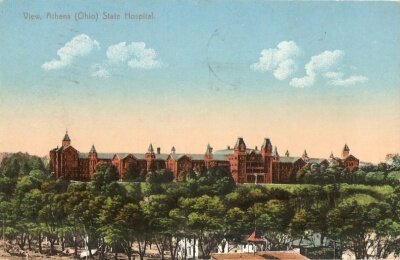
The Athens State Hospital was originally designed in 1867 by Ohio architect Levi Scofield according to the Kirkbride Plan. The grounds were later expanded according to the Cottage Plan by Frank Packard.

The Massillon State Hospital is a prime example of a facility designed (by Frank Packard) according to the Cottage Plan.